Volume 6 (2023) Issue 1 No.3 Pages 11-17
Abstract
Background and Purpose: This study aimed to identify patient motivation for physical activity before and after allogeneic hematopoietic stem cell transplantation (HSCT).
Methods: We conducted 14 semi-structured interviews of seven patients (two of each patient): one before starting a conditioning regimen and one after leaving the protected environment. All interviews were recorded and analyzed using the inductive content analysis method. The data collection period was May to December 2018.
Results: The participants comprised three men and four women aged 40-70 years. The patients underwent bone marrow, umbilical cord blood, or peripheral HSCT. The patients' motivation for physical activity before and after HSCT was classified into six categories and categorized into five themes including
Conclusions and implications for practice: The categories and themes developed here based on patient responses provide an important perspective that should be promoted among healthcare providers who care for patients undergoing HSCT.
Introduction
Hematopoietic stem cell transplantation (HSCT) can cure several hematological diseases and hematopoietic malignancies, such as leukemia, malignant lymphoma, and aplastic anemia. As of 2020, the annual number of HSCT cases in Japan surpassed 5,0001. The survival curves for allogeneic HSCT at 1 and 10 years after HSCT in Japan are 64.9% and 44.7%, respectively, and half of all allogeneic HSCT procedures are performed in patients aged >50 years. Bone marrow transplantation has good therapeutic effects, and the number of patients undergoing HSCT is expected to increase.
While patients undergoing allogeneic HSCT benefit from advances in therapeutic technology, they also experience adverse events such as general fatigue, digestive symptoms, infections, and graft-versus-host disease (GVHD) after HSCT, which significantly limits their physical activity2,3. In this context, disuse syndrome often develops in a protective environment due to decreased cardiopulmonary and cognitive function, depression, declining muscle and physical strength due to long-term inactivity, and sarcopenia4. Sarcopenia reportedly contributes to higher nonrelapse and all-cause mortality rates after allogeneic HSCT5. Patients undergoing allogeneic HSCT must minimize loss of physical function to prevent disuse syndrome. However, physical activity decreases significantly because of mucosal damage from pre-transplant chemotherapy, fever caused by infection, acute GVHD, use of steroids for preventing GVHD, and persistent fatigue after transplantation6,7. As a result, physical function declines after HSCT and voluntary engagement in physical activity becomes extremely difficult. Therefore, patient motivation for rehabilitation gradually declines, and some patients cannot maintain their usual physical activity. Hence, motivation can play a key role in encouraging patients to engage in physical activity and continue rehabilitation8,9. However, few studies have specifically identified the motivation behind physical activity among patients before and after allogeneic HSCT10,11. Therefore, here we aimed to elucidate the importance of motivation for physical activity among patients before and after HSCT and how it can contribute to physical and psychological support for patients undergoing HSCT.
Patients and Methods
Study design
This study used a qualitative descriptive approach to determine what motivates patients undergoing HSCT to be physically active.
Definition of physical activity
The World Health Organization defines physical activity as any bodily movement produced by the skeletal muscles that requires energy expenditure12. Therefore, in this study, we included the activities performed during the rehabilitation of patients undergoing HSCT as well as their daily physical activities.
Setting and participants
Participants were recruited from a university hospital situated in a rural area of Japan. Participants were included in the study if they met the following eligibility criteria: age >20 years, scheduled for HSCT to treat hematological disease, Eastern Cooperative Oncology Group Performance Status Scale (ECOG PS)13 0-1 in the hospital, no serious complications, and participation approved by the primary care physician. Written informed consent was obtained from all patients. A hematologist identified the potentially eligible patients and explained the study outline. If the patient was interested in participating, the hematologist referred them to a nursing investigator, who explained the study contents to those who met the inclusion criteria using an explanatory document. Each participant provided written informed consent. On the day of the interview, the nursing investigator explained the purpose and outline of the study to the patients once again and re-confirmed that they could opt out at any time after the interview.
Rehabilitation was performed before and after HSCT at the study facility. All participants were instructed by their physicians to undergo rehabilitation and did so throughout their hospital stay. The rehabilitation program included exercise instruction by a physical therapist that included stretching, strengthening exercises, and walking as well as pre- and post-transplant muscle strength assessments and a 6-minute walk test, all of which were tailored to the patient's condition.
Data collection
Two oncology nursing researchers (>5 years of experience in hematology nursing) developed an interview guide and ascertained at the first interview whether each participant could describe their personal perspectives. One of the nurses conducted semi-structured interviews using open-ended questions. Interviews were conducted twice: before (1-2 weeks from hospitalization to the start of the preparative transplant regimen) and after (1-2 weeks after leaving the protected environment room) HSCT. Fourteen interviews were conducted of the seven participants. None of the participants refused to be interviewed.
Motivation for physical activity is thought to differ before versus after HSCT, while physical activity is thought to decrease after HSCT. Therefore, it is beneficial to understand how HSCT patients balance their physical symptoms and physical activity before versus after HSCT. After leaving the protected environment room, the patients were interviewed within 1-2 weeks according to their physical condition. The main questions in the interview guide were as follows: 1) What is your motivation for physical activity? 2) What are your motivations for engaging in physical activity? The interviews were recorded digitally and transcribed. The mean interview duration was 42 minutes (range, 18-62 minutes) before starting the transplant preparative regimen and 22 minutes (range, 10-45 minutes) after leaving the protective environment. The interviews were conducted at a university hospital between May and December 2018.
Analysis
Interview data were analyzed using Graneheim and Lundman's content analysis14 as follows: 1) All interviews were recorded and transcribed and their content analyzed verbatim; 2) The oncology nursing researcher listened to the recordings and reviewed the transcripts to identify meaningful units; 3) The oncology nursing researcher extracted the units associated with the study topics, such as motivation for physical activity, in the form of initial codes; 4) The oncology nursing researcher conceptualized and categorized the extracted types of motivation for direct physical activity based on similarities and differences in content under the supervision of a cancer nursing investigator. Pre-HSCT data were first analyzed, followed by post-HSCT data; 5) The oncology nursing researcher integrated all categories before and after HSCT and then categorized them based on their similarities; 6) All categories of motivation for physical activity were defined; 7) Themes were defined from all categories; and 8) Surface validation for all categories and themes were performed by nurses with at least 5 years of experience in hematology. All interviews were conducted in Japanese, and DeepL software was used to perform English-to-Japanese-to-English translation.
Ethics approval
The study protocol was approved by the ethics committee of the Tokushima University Hospital (no. 3143) and performed in accordance with the latest version of the Helsinki Declaration. Seven patients received information pamphlets and provided written informed consent before the interviews, which were conducted in a private room. The physical status of each patient was considered, and interviews were promptly conducted by the researcher.
Results
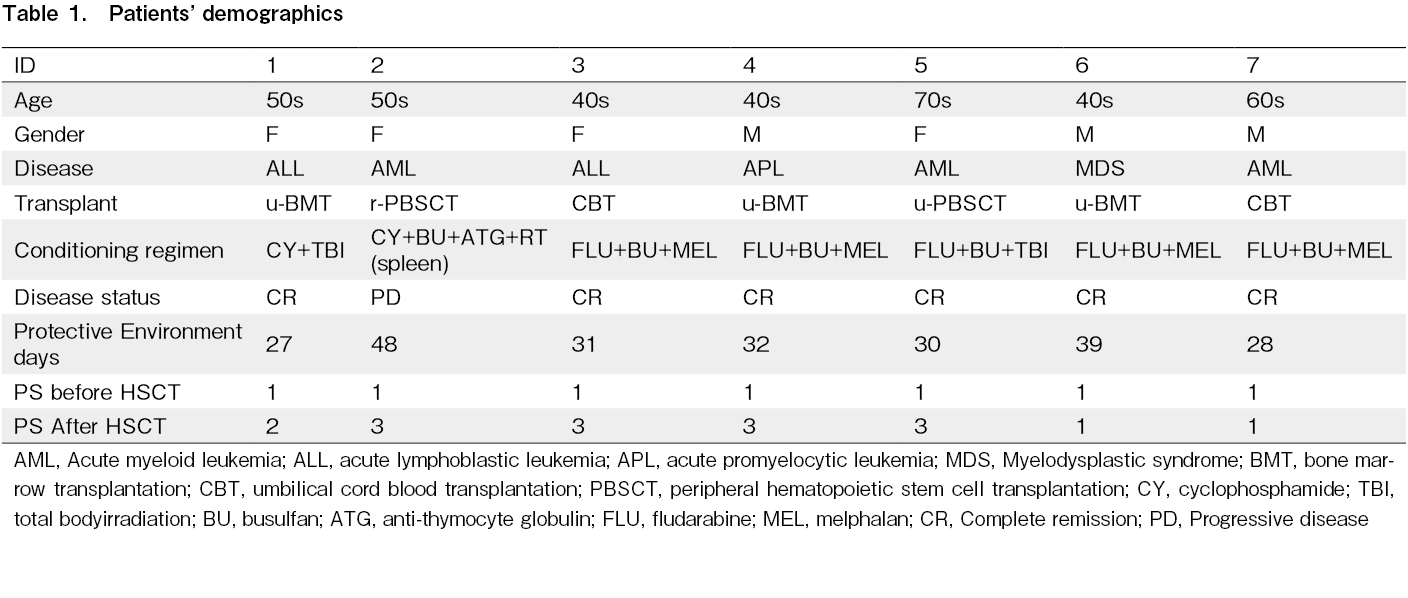
The participating patients comprised three men and four women aged 40-70 years (Table 1). The mean
Motivation for physical activity
The motivation for physical activity among patients before versus after HSCT was classified into six categories, from which five themes were derived. The categories are described below for each of the five themes:
“ To overcome HSCT”
Before HSCT
After HSCT
“ To look after myself”
Indicated that the patient was motivated by the desire to perform personal activities independently, particularly the desire to use the bathroom or take a shower on their own.
Before HSCT
After HSCT
“ To respond to the donor”
Indicated that the donor's presence was the reason behind the patients' hopes and desires to perform physical tasks as before HSCT. Their willingness to respond to the donor's feelings motivated them to perform physical activity.
Before HSCT
Having a family member as a donor was a significant source of emotional support.
“ The existence of supporters”
Indicates that patients were motivated by the presence of trusted medical professionals as well as people with the same disease who could share their transplant experience. This encouraged them to move independently. The presence of a supporter had a significant influence on patients' willingness to engage in physical activity.
Before HSCT
After HSCT
“ Encouragement from supporters”
Family members, health care providers, survivors, and other supporters of patients undergoing HSCT encouraged them to continue performing physical activity. The approval of healthcare professionals who understood the patients, as well as letters and photographs of the patients' children, gave them the strength they needed to stay motivated.
Before HSCT
After HSCT
Discussion
Desire to survive
One motivation for patients undergoing HSCT was
Another patient stated,
Self-esteem
The theme
Existence of supporters
Patients are unable to move after transplantation despite their desire due to various symptoms. At that time, as parents, the words of their child,
The presence of family members, healthcare providers, and peers can empower patients to continue engaging in painful physical activity. In particular, nurses should actively seek cooperation from the hematologist, as explanations from them will facilitate physical activity10.
Positive feedback from other HSCT survivors also promotes physical activity, and it is important to provide a place where people with the disease can communicate with each other10,11. Sharing the transplant experience with peers can help create a positive perception of one's own existence and aid the overcoming of transplant-related challenges. As it is difficult to maintain motivation for physical activity, encouragement from family members and medical personnel is essential.
Relevance for clinical practice
Physical activity effectively improves fatigue after HSCT, and various programs have been proposed21,22. Previous studies reported that before transplantation is the optimal time to begin exercise in preparation for HSCT23. However, few patients voluntarily exercise before HSCT in anticipation of their post-transplantation physical condition. Healthcare providers should clarify the purpose of pre- and post-transplant physical activity for HSCT patients and work with them accordingly. We recommend the following three nursing perspectives to promote physical activity motivation among transplant patients:
1) The physical activity of HSCT patients is strongly motivated by
2) The principle of nursing is to help patients maintain their self-esteem in all circumstances. Self-esteem motivates transplant patients to be physically active; however, it is also true that self-care ability declines significantly before and after transplantation. Therefore, supporting the patient's motivation to perform physical activity while providing appropriate support for their self-care ability is important.
3) For transplant patients, the presence of supporters motivates physical activity. During the transplant treatment process, direct infection control visits and contact with medical professionals are limited because maintaining minimal human interaction is an important aspect of care. In particular, the presence of family members was significant in this study; therefore, it is important to provide support in cooperation with family members.
Limitations
This study had several limitations. First, it was an interview-based survey conducted at one institution and included only seven subjects. Therefore, more cases require study in a similar manner. Second, all patients in this study talked about their motivation for physical activity, and it is possible that the study was biased toward those who were highly interested. Third, the results of this study do not clarify how to motivate patients to perform or maintain physical activity. Fourth, complications after transplantation occur frequently, and many patients in this study developed complications. Since the presence of physical symptoms influences the motivation for physical activity, further studies that consider complications are needed of the motivation for physical activity.
Conclusion
Motivations for physical activity were identified as follows:
Acknowledgments
The authors would like to thank all patients who willingly participated in this study, especially during the difficult period right before and after the transplant. We would like to thank Ms. Kumi Kimura of the Cell Therapy Center at the Tokushima University Hospital. This research could not have been accomplished without financial support from Yasuda Memorial Medical Foundation in Japan. We would like to thank Editage (www.editage.com) for the English language editing.
Author Contributions
K.N., S.F., R.Y., and C.O designed the study. K.N. collected the data. K.N. and C.O. analyzed the data.
Acknowledgments
The authors would like to thank all patients who willingly participated in this study, especially during the difficult period right before and after the transplant. We would like to thank Ms. Kumi Kimura of the Cell Therapy Center at the Tokushima University Hospital. This research could not have been accomplished without financial support from Yasuda Memorial Medical Foundation in Japan. We would like to thank Editage (www.editage.com) for the English language editing.
Financial Support
Yasuda Memorial Medical Foundation
Acknowledgments
The authors would like to thank all patients who willingly participated in this study, especially during the difficult period right before and after the transplant. We would like to thank Ms. Kumi Kimura of the Cell Therapy Center at the Tokushima University Hospital. This research could not have been accomplished without financial support from Yasuda Memorial Medical Foundation in Japan. We would like to thank Editage (www.editage.com) for the English language editing.
Ethics Approval
The study protocol was approved by the ethics committee of the Tokushima University Hospital (No.3143) and was performed in accordance with the latest version of the Helsinki Declaration.
Acknowledgments
The authors would like to thank all patients who willingly participated in this study, especially during the difficult period right before and after the transplant. We would like to thank Ms. Kumi Kimura of the Cell Therapy Center at the Tokushima University Hospital. This research could not have been accomplished without financial support from Yasuda Memorial Medical Foundation in Japan. We would like to thank Editage (www.editage.com) for the English language editing.
Consent for Publication
Seven patients received information pamphlets and provided written informed consent before the interviews, which were conducted in a private room. The physical status of each patient was considered, and interviews were promptly conducted by the researcher.
Conflicts of Interest
The authors declare no conflict of interest. Disclosure forms provided by the authors are available on the website.
References
1.The Japanese Data Center for Hematopoietic Cell Transplantation/The Japanese Society for Transplantation and Cellular Therapy. Hematopoietic cell transplantation in Japan. Annual report of nationwide survey 2021; https://www.jdchct.or.jp/en/data/slide/2021/ [Accessed: 6 October 2022]
2.Bevans MF, Mitchell SA, Marden S. The symptom experience in the first 100 days following allogeneic hematopoietic stem cell transplantation (HSCT). Support Care Cancer. 2008; 16: 1243-54.
3.Gielissen MF, Schattenberg AV, Verhagen CA, Rinkes MJ, Bremmers ME, Bleijenberg G. Experience of severe fatigue in long-term survivors of stem cell transplantation. Bone Marrow Transplant. 2007; 39: 595-603.
4.Tanaka S, Imataki O, Kitaoka A, Fujioka S, Hanabusa E, Ohbayashi Y, et al. Clinical impact of sarcopenia and relevance of nutritional intake in patients before and after allogeneic hematopoietic stem cell transplantation. J Cancer Res Clin Oncol. 2017; 143: 1083-92.
5.Ando T, Fujisawa S, Teshigawara H, Matsumura A, Sakuma T, Suzuki T, et al. Computed tomography-defined sarcopenia: Prognostic predictor of nonrelapse mortality after allogeneic hematopoietic stem cell transplantation: A multicenter retrospective study. Int J Hematol. 2020; 112: 46-56.
6.Lee HJ, Oran B, Saliba RM, Couriel DM, Shin K, Massey P, et al. Steroid myopathy in patients with acute graft-versus-host disease treated with high-dose steroid therapy. Bone Marrow Transplant. 2006; 38: 299-303.
7.Morishita S, Kaida K, Yamauchi S, Sota K, Ishii S, Ikegame K, et al. Relationship between corticosteroid dose and declines in physical function among allogeneic hematopoietic stem cell transplantation patients. Support Care Cancer. 2013; 21: 2161-9.
8.Pinto BM, Ciccolo JT. Physical activity motivation and cancer survivorship. Recent Results Cancer Res. 2011; 186: 367-87.
9.Jepsen LØ, Friis LS, Hoybye MT, Marcher CW, Hansen DG. Rehabilitation during intensive treatment of acute leukaemia including allogenic stem cell transplantation: A qualitative study of patient experiences. BMJ Open. 2019; 9: e029470.
10.Yu MS, An KY, Byeon J, Choi M, Cheong JW, Courneya K, et al. Exercise barriers and facilitators during hematopoietic stem cell transplantation: a qualitative study. BMJ Open. 2020; 10: e037460.
11.Abo S, Parry SM, Ritchie D, Sgro G, Truong D, Denehy L, et al. Exercise in allogeneic bone marrow transplantation: a qualitative representation of the patient perspective. Support Care Cancer. 2020; 30: 5389-99.
12.Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020; 54: 1451-62.
13.Japan Clinical Oncology Group. Common Toxicity Criteria, Version 2.0. 1999; http://www.jcog.jp/doctor/tool/ps.html [Accessed: 6 October 2022]
14.Graneheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004; 24: 105-12.
15.Mori K. Development of a nursing intervention program to support intrinsic motivation-based decision making by patients undergoing hematopoietic stem cell transplantation. Journal of Japanese Society of Cancer Nursing. 2008; 2: 55-64.
16.Tonosaki A. Impact of walking ability and physical condition on fatigue and anxiety in hematopoietic stem cell transplantation recipients immediately before hospital discharge. Eur J Oncol Nurs. 2012; 16: 26-33.
17.Miyashita M, Sanjo M, Morita T, Hirai K, Uchitomi Y. Good death in cancer care: a nationwide quantitative study. Ann Oncol. 2007; 18: 1090-7.
18.Ribeiro Nunes Lages SM, Ferreira Emygdio R, Sampaio Irene Monte A, Alchieri JC. Motivation and self-esteem in university students' adherence to physical activity. Rev Salud Publica. 2015; 17: 677-88.
19.Yap CC, Mohamad Som RB, Sum XY, Tan SA, Yee KW. Association between self-esteem and happiness among adolescents in Malaysia: The mediating role of motivation. Psychol Rep. 2022; 125: 1348-62.
20.Yang Y, Pan W, Farag SS, Von Ah D. Effect of family cohesion on symptom distress during hematopoietic stem cell transplantation. Support Care Cancer. 2022; 30: 1731-7.
21.Brassil KJ, Szewczyk N, Fellman B, Neumann J, Burgess J, Urbauer D, et al. Impact of an incentive-based mobility program, “Motivated and Moving,” on physiologic and quality of life outcomes in a stem cell transplant population. Cancer Nurs. 2014; 37: 345-54.
22.Kisch A, Jakobsson S, Forsberg A. Implementing a feasible exercise programme in an allogeneic haematopoietic stem cell transplantation setting-impact on physical activity and fatigue. Int J Environ Res Public Health. 2020; 17: 4302.
23.Liang Y, Zhou M, Wang F, Wu Z. Exercise for physical fitness, fatigue and quality of life of patients undergoing hematopoietic stem cell transplantation: A meta-analysis of randomized controlled trials. Jpn J Clin Oncol. 2018; 48: 1046-57.
Search
News


