Volume 6 (2023) Issue 4 No.3 Pages 124-128
Abstract
Introduction: While there are data about return to work after hematopoietic cell transplantation (HCT) in survivors from resource-rich regions, similar data from resource-challenged settings are scarce. This study assessed the incidence of and factors affecting return to work/school (RTW) among HCT survivors in India.
Methods: This single-center cross-sectional study was conducted at the long-term follow-up (LTFU) clinic of a large-volume HCT center during 2022-2023. HCT survivors surviving beyond four months were included after obtaining informed consent. Patients' sociodemographic, disease, HCT, and work details were recorded. The factors affecting RTW were evaluated using univariate (ANOVA) and logistic regression analyses.
Results: A total of 126 HCT survivors participated in the study. Of these, 34 (27%) did not RTW, 47 (37%) returned to part-time work, and 45 (36%) returned to full-time work at a median of more than three years post-HCT. The three groups did not significantly differ in age, sex, or marital status. The univariate analysis revealed that education, pre-HCT job status, income, and conditioning intensity were significantly associated with RTW. Logistic regression analysis revealed that survivors with a higher (taxable) income were more likely to RTW than those with a lower (non-taxable) income (OR 3.5; CI 1.2-10.2, p=0.01). Survivors with a desk job were more likely to RTW than those who were unemployed/retired or students (OR 4.5; CI 1.1-18.0, p=0.03).
Conclusion: Socioeconomic factors, like pre-HCT job status and income, were significantly associated with post-HCT RTW. Therefore, there is a need to integrate multidisciplinary RTW programs for HCT survivors in India.
Introduction
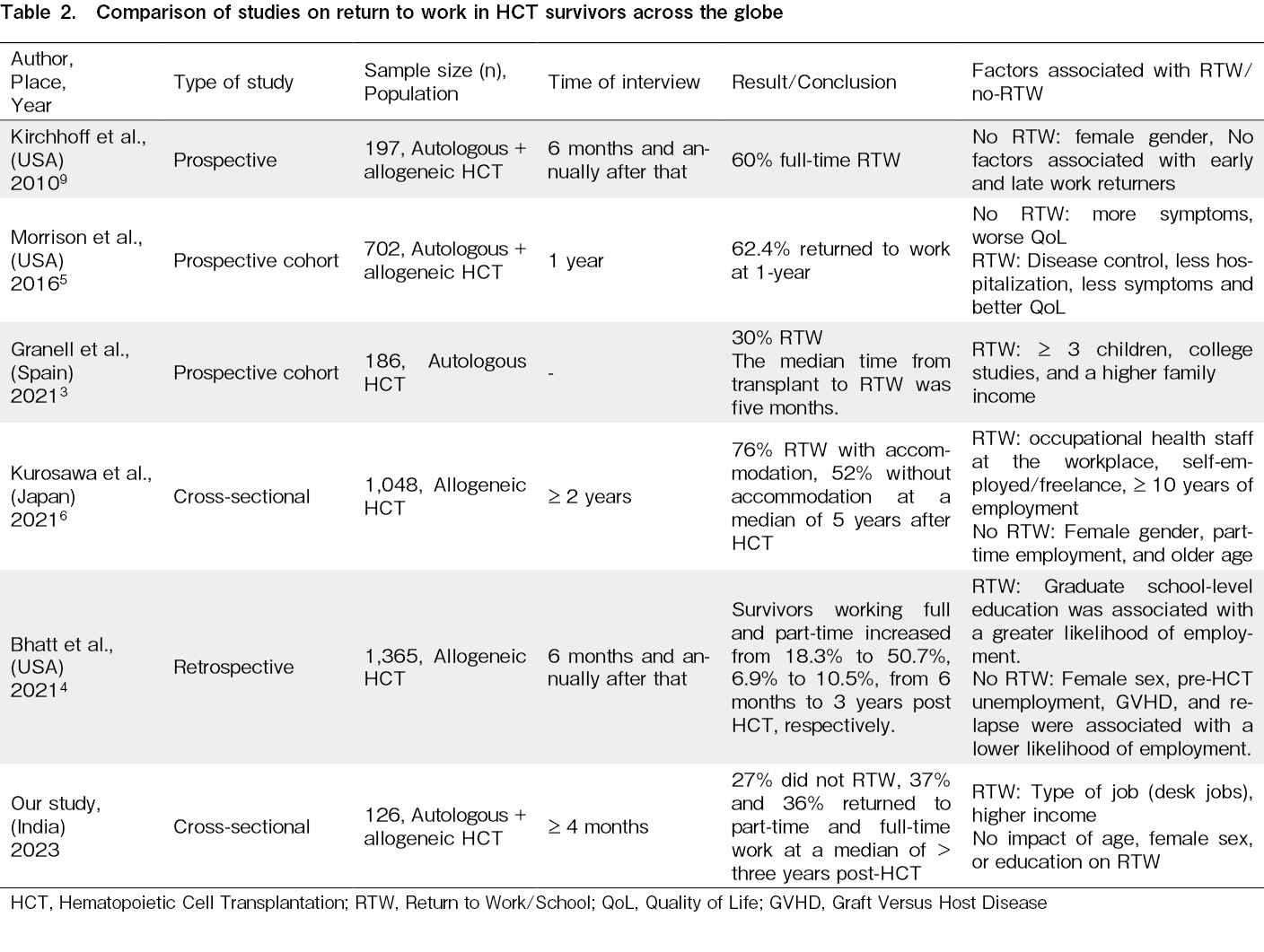
Return to work/school (RTW) and quality of life (QOL) after hematopoietic cell transplantation (HCT) are interdependent. We only have data from resource-rich regions about RTW, a vital survivorship care parameter. The percentage of recipients who were working at the time of HCT and RTW varies from 30-76% by region1–4, 5. In regions with high RTW (76%), the most typical time for resignation is after discharge post-HCT (46%), followed by resignation after the initial diagnosis (27%)6. However, long-term follow-up (LTFU) in most countries does not incorporate RTW advice. A survey of the Center for International Blood and Marrow Transplant Research (CIBMTR) centers showed that only 44% of centers had RTW guidelines, and only 36% had RTW programs incorporated into their LTFU care7. Data on return to school are even more limited. In particular, we need data about RTW from centers in India, where even data about LTFU are scarce8. With the increasing number of HCT survivors in India, more research is warranted on HCT recipients' experiences with RTW. For instance, the factors associated with RTW in India may differ from those in more resource-rich regions. This study assessed the incidence of RTW among HCT survivors in India and analyzed its associated factors.
Methods
This single-center cross-sectional study was conducted at the LTFU clinic of a large-volume HCT center in North India during 2022-2023. HCT survivors surviving beyond four months were included after obtaining informed consent. This study was approved by the Institutional Ethics Committee. Sociodemographic, disease, and treatment information, including HCT parameters for all recipients, were available at baseline. Additional work/school-related information, including RTW, was acquired at the follow-up. For the analysis, we broadly classified work into three categories based on the physical work required: school/unemployed/retired, desk jobs, and field/business/homemakers. Any RTW at less than the pre-HCT levels, as perceived by the recipients, was classified as part-time RTW. Factors affecting RTW (no versus part-time versus full-time) were evaluated using univariate (ANOVA) and binary logistic regression analyses (no RTW versus RTW).
Results
A total of 126 HCT survivors participated in this study. Of these, 34 (27%) did not RTW, 47 (37%) returned to part-time work, and 45 (36%) returned to full-time employment. All three patient cohorts were matched for age (median 40 versus 41 versus 37 years, respectively; p=0.5) (Table 1). The median follow-up post-HCT was also similar (3.6 versus 3.1 versus 3.5 years, respectively; p=0.5). The proportions of males/females and single/married individuals in all three cohorts were similar (p=0.6 and 1.0, respectively). However, the cohorts significantly differed on socio-economic parameters such as education, pre-HCT jobs, primary wage earners, and income. Having graduate or higher education was associated with a higher RTW than being illiterate or a school student (60% versus 40% for part-time, and 78% versus 22% for full-time, p=0.01). Survivors with desk jobs were more likely to RTW full-time (47%), and those with field/business/homemakers were more likely to RTW part-time (47%) than school-going/unemployed or retired survivors, who were more likely to not RTW (47%) (p=0.001). Survivors who were dependent on other family members and earning less than the taxable income were more likely to not RTW compared to those who were self-wage earners (74% versus 26%, p=0.03) and had a higher income at the time of diagnosis (82% versus 18%, p=0.001). Funding for HCT (private/government or out-of-pocket), disease diagnosis, and type of HCT (autologous or allogeneic) did not affect RTW. However, survivors receiving myeloablative conditioning were less likely to RTW than those receiving reduced-intensity/non-myeloablative conditioning (97% versus 3%, p=0.03). Moderate-to-severe chronic graft versus host disease (GVHD) did not affect RTW.
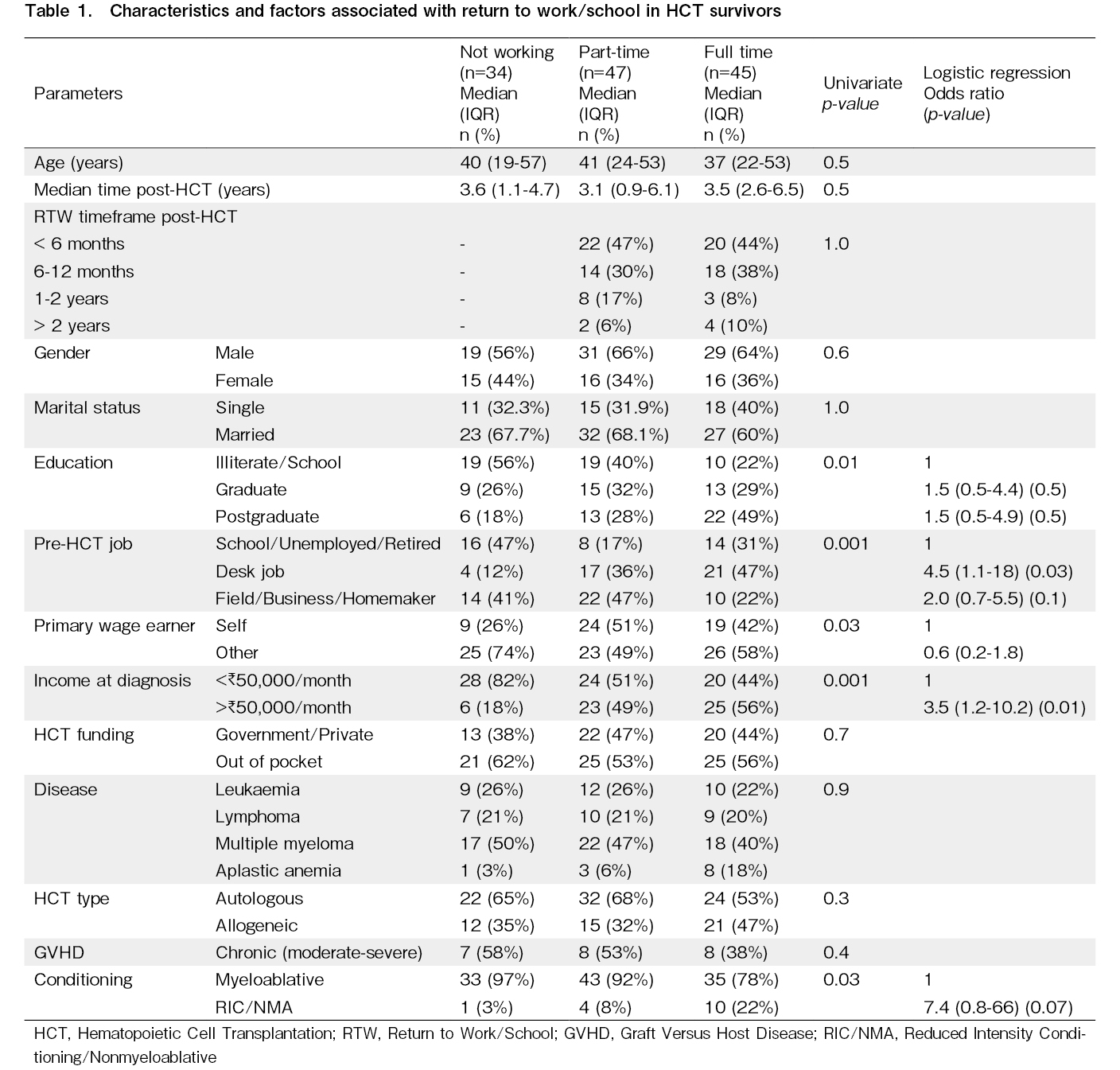
The binary logistic regression analysis comparing those who did and did not RTW revealed that survivors with a higher (taxable) income were more likely to RTW than survivors with a lower (non-taxable) income (OR 3.5; CI 1.2-10.2, p=0.019). Survivors with a desk job were more likely to RTW than those who were already unemployed/retired or a student (OR 4.5; 1.1-18.0, p=0.030). Education level, primary wage status, and conditioning regimen intensity were not significant factors.
We further analyzed the reasons for RTW (or not). 65% of those who did not RTW cited their health status and precautions. Other reasons (32%) included psychosocial, wanting to spend time with family, and spiritual factors. Only one patient reported not finding a job as a reason for not RTW. Of those who RTW, the majority (80%) returned to the same work within a year post-HCT; 87% mentioned having a flexible and supportive workplace environment.
Discussion
Although most HCT providers recognize the need for RTW guidance for HCT survivors, only a small proportion receive it7. This has prompted the American Society for Transplantation and Cellular Therapy (ASTCT) to provide RTW recommendations to HCT providers recently1. These guidelines recommend a multidisciplinary collaborative approach involving HCT physicians, psychologists, social workers, occupational therapists, physiotherapists, vocational counselors, and nurses for RTW plans. However, we need crucial data on the incidence of and factors associated with RTW to provide appropriate guidance in resource-challenged regions. Our study shows that 73% of HCT survivors RTW either part- or full-time at a median of more than three years. Only a quarter could not RTW. These proportions are encouraging, given that only approximately 50-60% achieved RTW in resource-rich economies7. Surprisingly, most patients returned to the same work and reported a flexible and supportive work environment. Except for the Japanese study that showed that occupational health staff at the workplace was associated with RTW, little is known about workplace adaptability6.
Our study found that the type of pre-HCT job (desk job) and higher income were motivators for RTW. This is consistent with studies from resource-rich regions worldwide2, 3, 6 (Table 2). However, the only factor that is different in our study is the lack of impact of being a female on RTW, which is in contrast to other studies reporting it as a factor associated with no RTW. This may be because we included homemakers as a category; the support system of Indian families encouraged homemakers to return to at least partial work after HCT. We also found no difference in RTW by HCT type, conditioning regimen, or GVHD, consistent with previous studies5, 9. The limitations of our study include its cross-sectional design and the lack of a correlation between QoL and disease remission status. In addition, given the small numbers, we did not separately analyze homemakers and return to school from RTW, which makes our RTW definition unique. Since work hours are not defined in any Indian workplace, we relied on patients' perceptions of RTW of part- or full-time employment. The job of an Indian homemaker is a full-time endeavor involving hard labor, as most homemakers are involved in tasks related to cooking, cleaning, laundry, and shopping for household essentials and groceries. Given the ASTCT's recommendations for RTW guidance in resource-rich regions, we need to adapt these recommendations to resource-challenged areas without access to all multidisciplinary staff. Finally, the flexibility of Indian workplaces was encouraging. In collaboration with medical social workers, HCT providers should guide the vocational rehabilitation of all HCT survivors. This study serves to sensitize HCT teams in India to this vital survivorship care parameter and incorporate RTW plans into their LTFU care.
Author Contributions
AP and UB contributed equally. AP, UB, PM, and DPL contributed to the study conception and design. All authors performed data collection and analysis. AP, UB, and DPL wrote the first draft of the manuscript, and all authors commented on previous versions. All authors read and approved the final manuscript.
Ethics Approval
The study was cleared by the institutional ethics committee, PGIMER, NK/7391/Study/851.
Informed consent
Informed consent was obtained from all participants included in the study.
Funding Statement
The American Society of Hematology (ASH) Global Research Award to DPL partly funded the study.
Conflicts of Interest
The authors declare no conflict of interest. Disclosure forms provided by the authors are available on the website.
References
1.Salit RB, Schoeppner K, De Biase C, Mohammed J, Gonzales AL, Hashmi SK, et al. American society for transplantation and cellular therapy return to work guidance committee recommendations for health care providers who take care of hematopoietic cell transplantation patients. Transplant Cell Ther. 2022; 28: 822-8.
2.Bhatt NS, Brazauskas R, Salit RB, Syrjala K, Bo-Subait S, Tecca H, et al. Return to work among young adult survivors of allogeneic hematopoietic cell transplantation in the united states. Transplant Cell Ther. 2021; 27: 679.e1-8.
3.Granell M, Senín A, Barata A, Cibeira MT, Gironella M, López-Pardo J, et al. Predictors of return to work after autologous stem cell transplantation in patients with multiple myeloma. Bone Marrow Transplant. 2021; 56: 2904-10.
4.Bhatt NS. Prevalence and Determinants of Return to Work as a Patient-Centered Outcome in Survivors of Hematopoietic Cell Transplantation. Curr Hematol Malig Rep. 2022; 17: 228-42.
5.Morrison EJ, Ehlers SL, Bronars CA, Patten CA, Brockman TA, Cerhan JR, et al. Employment Status as an Indicator of Recovery and Function One Year after Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant. 2016; 22: 1690-5.
6.Kurosawa S, Yamaguchi T, Mori A, Matsuura T, Mori T, Tanaka M, et al. Resignation and return to work in patients receiving allogeneic hematopoietic cell transplantation close up. J Cancer Surviv. 2022; 16: 1004-15.
7.Salit RB, Lee SJ, Burns LJ, Shaw BE, Majhail NS, Bhatt NS, et al. Return-to-Work Guidelines and Programs for Post-Hematopoietic Cell Transplantation Survivors: An Initial Survey. Biol Blood Marrow Transplant. 2020; 26: 1520-6.
8.Khaire NS, Chhabra P, Gupta DG, Jandial A, Khadwal A, Kasudhan KS, et al. Adherence to long-term follow-up preventive practices in allogeneic hematopoietic cell transplantation survivors from North India. Blood Cell Ther. 2022; 5: 83-6.
9.Kirchhoff AC, Leisenring W, Syrjala KL. Prospective predictors of return to work in the 5 years after hematopoietic cell transplantation. J Cancer Surviv. 2010; 4: 33-44.
Search
News


